

- 3.10 MB
- 2022-04-29 14:39:04 发布
- 1、本文档共5页,可阅读全部内容。
- 2、本文档内容版权归属内容提供方,所产生的收益全部归内容提供方所有。如果您对本文有版权争议,可选择认领,认领后既往收益都归您。
- 3、本文档由用户上传,本站不保证质量和数量令人满意,可能有诸多瑕疵,付费之前,请仔细先通过免费阅读内容等途径辨别内容交易风险。如存在严重挂羊头卖狗肉之情形,可联系本站下载客服投诉处理。
- 文档侵权举报电话:19940600175。
'心房颤动的治疗新的循证医学证据——英文课件
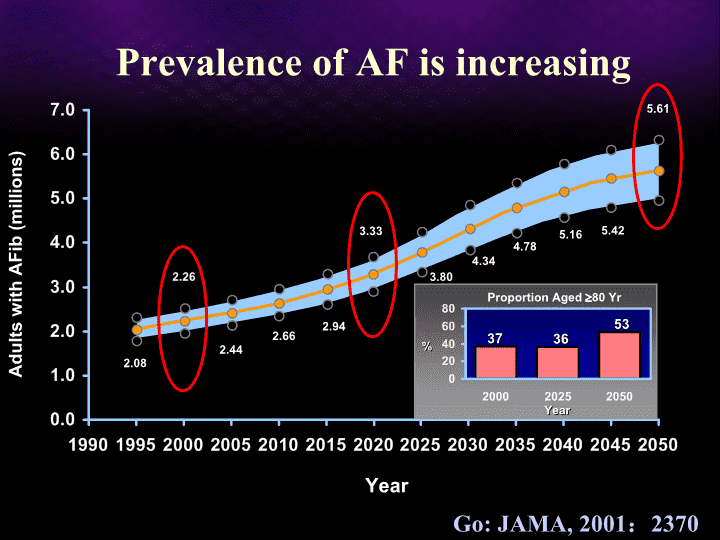
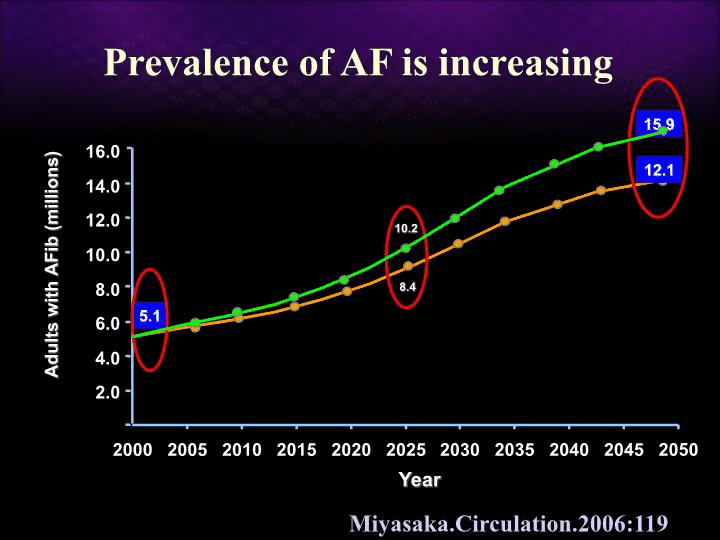
PrevalenceofAFisincreasingAdultswithAFib(millions)Year2.082.262.442.662.943.333.804.784.345.165.425.61%363753YearProportionAged80YrGo:JAMA,2001:2370
Realworldofwarfarinintheelderly13.1%4.7%Thefirst90daysassociatedwithmajorhemorrhage21%ptswithdrawnwarfarinforsafetyissueThehigherriskofstroke,thehigherincidenceofmajorhemorrhageHylek.Circulation.2007,2689
HRforICHwas4.06forAsiansAsianswereatgreaterriskforwarfarin-ralatedICHShen.JACC.2007:309
Prospective,randomize,control973pts≽75yearsoldwithAFRandomizedintowarfarinarm(INR2.0-3.0)andAspirinarm(75mg/d)MeanF/U2.7yrsPrimaryoutcome:fatalordisablingstroke,intracranialhaemorrhage,orarterialembolismWarfarinversusaspirinforstrokepreventionintheelderlywithAF(TheBirminghamAtrialFibrillationTreatmentoftheAgedStudy,BAFTAstudy)Mant.Lancet,2007,493
0.831.155(0.4%)6(0.5%)haemorrhagic0.651.921(0.1%)2(0.2%)OtherICH0.360.323(0.2%)1(0.1%)Embolism48(3.8%)7(0.5%)32(2.5%)23(1.8%)21(1.6%)44(3.4%)0.0050.338(0.6%)disablingnonfatal0.00270.4824(1.8%)Total0.530.695(0.4%)unknown0.00040.3010(0.8%)ischemic0.140.5913(1.0%)fatal0.0030.4621(1.6%)StrokepEventwarfarin(n=488)ASA(n=488)N(Riskperyear)N(Riskperyear)warfarinVS.ASARRWarfarinversusaspirinforstrokepreventionintheelderlywithAFMant.Lancet,2007,493
Mant.Lancet,2007,493WarfarinversusaspirinforstrokepreventionintheelderlywithAF
Anticoagulationinclinicalpractice2.03/100person-yrs1.17/100person-yrs11,526ptswithAF,54.8%wasonwarfarinRelativeriskforthromb-embolismreduced51%inwarfarintherapyTheintracranialhemorrhagerateincreasedinwarfarin(0.46/100person-yrsVS0.23/100person-yrs)Warfarinwasnotassociatedwithnonintracranialhemorrhage(1.05/100person-yrsVS1.06/100person-yrs)Go.JAMA2003:2685
RivaroxabanEnoxaparin873ptsEndpointsincludedDVT,PE,allcausemortalitySafety:majorhemorrhageEndpointsSafetyEriksson.Circulation.2006:2374%Rivaroxaban—Newpromiseofanticoagulation?
ProspectiveRIKS-HIA60764pts,AF21459pts,CHF22345pts,AF+CHF16960ptsF/U1yrHighermortalityrateinAFwithoutCHFptstakingdigoxin(RR1.42)SimilarmortalityrateinCHForAF+CHFptswithorwithoutdigoxinDigoxinandmortalityinAF:AprospectivecohortstudyHallberg.EuroJClinPharmacol,2007,959
Hallberg.EuroJClinPharmacol,2007,959DigoxinandmortalityinAF:Aprospectivecohortstudy
AdverseeffectsoforalamiodaroneZimetbaum.NEJM.2007:935Bradycardia5%ProlongedQTInmostTdp<1%Hepatic15%Hyperthyroidism3%Hypothyroidism20%Pulmonary<3%Dermatology25-75%Neurologic3-30%Cornealdeposits100%Opticneuritis<1%
NicholG.Heart.2002:535JAmCollCardiol.2003:20AADsisinsufficienttomaintainsinusrhythm
AmiodaroneincreasedmortalityofHFSCD-HeFT研究Bardy.NEJM,2005:225
Dronedarone:Substitutionofamiodarone?Derivativeofamiodarone,notcomposedofiodineEliminatetheeffectsofamiodaroneonthyroidandpulmonaryfunctionsHalf-time24hours22.6%discontinuationbecauseofGItractcomplicationsTouboul.PACE.2002:574(A)
64.1%75.2%DronedaroneformaintenanceofSRinAF:multicenter,double-blind,randomizedtrialsSingh.NEJM.2007,987
CatheterablationissuperiortoantiarrhythmicdurgAprospective,multicenter,randomized,controlledstudyablation+AADsAADs137AFpts(CAF33%)RandomizationCPVA+isthmusablationTranstelephonicECG,HolterF/U1yrAblation+AADsuccessrate55.9%SuccessrateofAADs8.7%Stabile.EurHeartJ.2006:216
APAFTrial29%Pappone.JACC.2006:2340198ptswithPAFRandomizationF/U1yrsSuccess:ATafree86%22%
Oral.NEJM.2006:934146CAFEventrecorderF/UCPVA:74%>AAD:4%
Catheterablationdecreasetheincidenceofstroke755ptsTheincidenceofstroke/TIAwas1.1%0.9%occurredwhithin2weeksofRFCA79%ofptswithoutriskfactorforstrokeand68%ofptswith≥1riskfactorinsinusdiscontinuedwarfarinPatientswithsinusrhythmwasthromboemboliceventfreeaftertheprocedureOral.Circulation.2006:759
Pappone.JACC.2003:185N=589N=582Catheterablationreducestroke
Pappone.JACC.2003:185Catheterablationimproveprognosis
Noriskfactor:ASA81-325mgOnemoderateriskfactor:ASA81-325mgorwarfarinAnyhighriskfactorormorethanonemoderateriskfactor:warfarinPrinciplesofanticoagulation
Amiodarone=Ablation!NoOHDyesHTNyes(concomitancwithLVHamiodarone>ablation)CADyesHFamiodarone>ablationMaintainSinusRhythmCatheterablationisareasonable alternativeto pharmacologicaltherapytopreventrecurrent AF(IIa,C)Fuster.Circulation.2006:e257
IndicationsforcatheterablationThepresenceofsymptomaticAFrefractoryorintoleranttoatleastoneClass1or3antiarrhythmicmedicationinrareclinicalsituations,itmaybeappropriatetoperformcatheterablationofAFasfirstlinetherapyselectedsymptomaticpatientswithheartfailureand/orreducedejectionfractionLAthrombusisacontraindicationHRS/EHRA/ECASExpertConsensusStatement
AFAblationasfirst-linetherapy?
(CatheterAblationvs.AntiarrhythmicDrugTherapy
forAtrialFibrillationTrial,CABANA)OngoingNIHsponsoredCABANAstudy:mortalitystudyofAFablationvs.antiarrhythmicsvs.ratecontrol/coumadinasfirst-linetherapyforAFMainstudytoenroll3,000patientsat100centersPatientswillbefollowedfor2.5-5years
ThankYou!
结束语谢谢大家聆听!!!34'
您可能关注的文档
- 最新心包疾病的诊断和治疗-课件PPT课件
- 最新心包疾病课件PPT课件
- 最新心境稳定剂的合理使用2 ppt课件PPT课件
- 最新心因性头晕的诊断治疗ppt课件PPT课件
- 最新心律失常 PPT课件PPT课件
- 最新心律失常-教学课件PPT课件
- 最新心律失常的概述课件PPTPPT课件
- 最新心律失常的诊断和治疗 PPT课件PPT课件
- 最新心律学新进展--心肺复苏PPT课件PPT课件
- 最新心灵快餐ppt课件PPT课件
- 最新心灵花园沙盘课件PPT课件
- 最新心灵花园Appt课件PPT课件
- 最新心理与教育测量第三章课件PPT课件
- 最新心理健康主题班会课件课件PPT课件
- 最新心理健康教育主题班会主题班会课件PPT课件
- 最新心理健康教育之学习篇1ppt课件PPT课件
- 最新心理健康课件PPT课件
- 最新心理励志心态培训ppt课件PPT课件